 |
Case Report
Adult case of slipped capital femoral epiphysis initially requiring in situ fixation with revision to total hip arthroplasty after failure of index surgery
1 MD, UCF/HCA Consortium, Resident, Graduate Medical Education Department of Orthopedic Surgery, HCA Florida Ocala Hospital, Ocala, FL, USA
2 DO, UCF/HCA Consortium, Resident, Graduate Medical Education Department of Orthopedic Surgery, HCA Florida Ocala Hospital, Ocala, FL, USA
3 MD, UCF/HCA Consortium, Attending Physician, Graduate Medical Education Department of Orthopedic Surgery, HCA Florida Ocala Hospital, Ocala, FL, USA
Address correspondence to:
Kyle Mahoney
MD, 514 NE 40th Ave, Ocala, FL 34470,
USA
Message to Corresponding Author
Article ID: 100029Z14KM2024
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Mahoney K, Lee-Norris A, Romero A, McFadden J. Adult case of slipped capital femoral epiphysis initially requiring in situ fixation with revision to total hip arthroplasty after failure of index surgery. J Case Rep Images Orthop Rheum 2024;7(1):1–4.ABSTRACT
Introduction: Slipped capital femoral epiphysis (SCFE) is a disorder classically associated with pediatric patients in which the femoral head is displaced through the physis. In rare cases of metabolic and hormonal disorders, SCFEs can be identified in adult patients as a result of persistent growth plates. Optimal definitive surgical management of these patients is still unknown and more information is needed in order to provide appropriate care for these patients.
Case Report: A 31-year-old male with past medical history of hypopituitarism presented with left hip pain after a seizure. He was found to have a left slipped capital femoral epiphysis on initial radiographs for which he was taken to the operating room for open treatment of the left SCFE with in situ screw fixation. Approximately four weeks later he returned to the hospital after a fall with left hip pain and inability to ambulate. Radiographs demonstrated cutout of the cannulated screw in the setting of a SCFE with further displacement. He returned to the operating room for conversion to an uncemented total hip arthroplasty. His post-op course was uneventful and he was discharged home in stable condition.
Conclusion: This cases highlights a condition uncommonly identified in adult patients which was further complicated by failure of the initial surgical repair and need for revision surgery. This case is unique in that total hip arthroplasty as a definitive treatment for acute SCFE, rather than treatment for end stage arthritis secondary to chronic SCFE, has not been reported upon this author’s review.
Keywords: Adult, Epiphysis, Hypopituitarism, Revision, Slipped
Introduction
Slipped capital femoral epiphysis (SCFE) is a condition in which there is subluxation of the femoral head relative to the femoral neck through the physis [1]. This is a condition that most commonly occurs in adolescents and has been associated with both mechanical and hormonal causes [2]. Mechanical causes include obesity, femoral retroversion, and increased physeal obliquity. Hormonal imbalance, such as in hypothyroidism, growth hormone supplementation, hypogonadal abnormalities, and hypopituitarism, results in physeal weakness that predisposes patients to SCFEs [3].
Despite the ample information available on adolescents with SCFEs, there is still little known on this disorder in the adult population. The authors present the case of an adult patient with hypopituitarism who developed a SCFE after a seizure which required in situ screw fixation followed by revision total hip arthroplasty after failure of the index procedure.
Case Report
The patient was a 31-year-old male with past medical history of hypopituitarism on chronic cortisone and levothyroxine therapy, anxiety, depression, attention deficit disorder, bipolar disorder, epilepsy, intellectual disabilities, and congenital septo-optic dysplasia complicated by left eye blindness. He presented to the emergency department with a chief complaint of left hip pain. The patient noted that he was unable to get his seizure medications the weekend prior to presentation and had two back to back seizures followed by left hip pain. He required a walker or cane in order to ambulate afterward. He denied any associated numbness, tingling, or weakness of the right lower extremity but noted decreased range of motion of the left hip secondary to pain.
Initial radiographs of the left hip demonstrated a slipped capital femoral epiphysis (SCFE) and evidence of skeletal immaturity (Figure 1A and Figure 1B). The patient’s physical exam was significant for mild tenderness of the left hip, moderate pain with passive internal and external rotation of the hip, and inability to flex and extend the hip due to pain. Neurological and vascular exams of the left lower extremity were within normal limits.
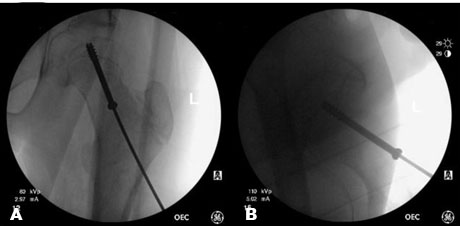
On hospital day two the patient was taken to the operating room for open treatment of the left SCFE with in situ screw fixation. Prior to surgery a discussion was had regarding use of a Femoral Neck System for fixation; however, given the large slip angle, fixation with cannulated screws was decided upon. A single 60 mm × 7.3 mm cannulated screw was used for fixation and its placement confirmed on multiple intra-operative fluoroscopic images (Figure 2A and Figure 2B). The patient’s post-operative course was uncomplicated and he was discharged home on post-op day one with home physical therapy. He was made partial weight bearing on the left lower extremity for four weeks before transitioning to full weight bearing. The patient was highly recommended to follow up with his endocrinologist for continued management of his hypopituitarism as well as for monitoring of his overall bone health.
The patient was seen at two weeks post-op and was noted to be doing well at that time. His staples were removed and he was recommended to continue home physical therapy.
On post-op day 42 the patient returned to the emergency department after a mechanical ground level fall. He noted he was making his bed when he lost his balance and had immediate onset of left hip pain. He reported constant pain since the index surgery but after his fall had inability to ambulate secondary to pain. He again denied any associated numbness, tingling, or weakness.
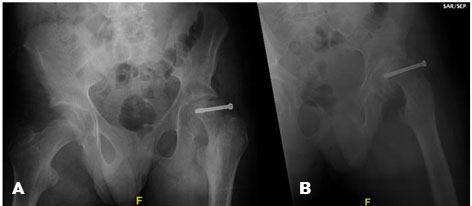
Radiographs at that time demonstrated cutout of the cannulated screw in the setting of a SCFE with further displacement (Figure 3A and Figure 3B). Physical exam was similar to his initial presentation.
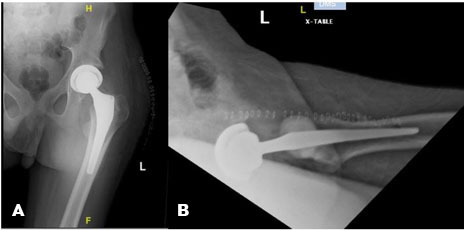
He returned to the operating room on hospital day three of his second admission for conversion of the prior left hip surgery to an uncemented total hip arthroplasty (Figure 4A and Figure 4B). He tolerated the procedure well and there were no complications. His post-op course was uneventful, and he was discharged home and stable condition on post-op day two. He was made full weight bearing on the left lower extremity immediately after surgery without issues.

Discussion
Slipped capital femoral epiphysis is a Salter-Harris Type I fracture that is most commonly seen in adolescent patients. These injuries can be seen from an abnormally high force transmitted across a normal physis, a normal force transmitted across a weakened physis, or a combination of the two [1]. However, this injury pattern in adult patients is more closely linked with the latter of these two mechanisms, as seen in the patient presented in this report [4],[5]. Witbreuk et al. summarized the effects of various endocrinopathies on hormonal signaling defects and the overall effect these have on the extracellular matrix of the physis. They discussed the complex, multifactorial Growth Hormone-Insulin Like Growth Factor-1 axis. Under normal conditions, this axis plays a role in forming the physis, but when it is not functioning correctly it can result in increased risk for developing SCFEs [3]. Tangible results of this study were reported in a case by Huang et al. in which an adult patient with congenital hypopituitarism developed a SCFE at the age of 29 which required operative fixation [6]. Finally, Macia-Villa et al. described the case of a 47-year-old female who presented with bilateral SCFEs after years of chronic inhaled corticosteroid use. They went on to expand their literature review and outlined 60 additional cases of SCFEs in patients >18 years old; the majority of which were associated with endocrine dysfunction, hypothyroidism, or hypogonadism [7],[8].
Conclusion
Although there has been some headway in identifying associations with adult SCFE, such as underlying metabolic or hormonal disorders, there is still a large gap in the medical knowledge regarding appropriate perioperative medical management as well as surgical management. In adults, in situ fixation, as compared to total hip arthroplasty as the index surgery, may not have the same efficacy as in pediatric populations.
REFERENCES
1.
Loder RT, Skopelja EN. The epidemiology and demographics of slipped capital femoral epiphysis. ISRN Orthop 2011;2011:486512. [CrossRef]
[Pubmed]

2.
Millis MB. SCFE: Clinical aspects, diagnosis, and classification. J Child Orthop 2017;11(2):93–8. [CrossRef]
[Pubmed]
3.
Witbreuk M, van Kemenade FJ, van der Sluijs JA, Jansma EP, Rotteveel J, van Royen BJ. Slipped capital femoral epiphysis and its association with endocrine, metabolic and chronic diseases: A systematic review of the literature. J Child Orthop 2013;7(3):213–23. [CrossRef]
[Pubmed]
4.
Moyer J, Jacks L, Hunter JD, Chan G. Slipped capital femoral epiphysis and associated hypothyroidism. A review of the literature with two classic case examples. J Pediatr Endocrinol Metab 2016;29(4):427–34. [CrossRef]
[Pubmed]
5.
Whyte N, Sullivan C. Slipped capital femoral epiphysis in atypical patients. Pediatr Ann 2016;45(4):e128–34. [CrossRef]
[Pubmed]
6.
Huang YF, Wang LS, Zhang S, Gao YH, Liu JG, Qi X. Slipped capital femoral epiphysis in an adult with congenital hypopituitarism: A case report. Medicine (Baltimore) 2019;98(3):e13997. [CrossRef]
[Pubmed]
7.
Macía-Villa CC, Sanchez-Lite I, Medina-Luezas J. Slipped capital femoral epiphysis in adults: Case report and review of literature. Reumatismo 2016;68(1):40–7. [CrossRef]
[Pubmed]
8.
Nelms NJ, Lewallen LW, McIntosh AL, Sierra RJ. Total hip arthroplasty in the young: Special emphasis on post-SCFE patients. J Pediatr Orthop 2013;33 Suppl 1:S137–42. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Kyle Mahoney - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Alexandria Lee-Norris - Conception of the work, Design of the work, Acquisition of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Andrew Romero - Conception of the work, Design of the work, Analysis of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
James McFadden - Conception of the work, Design of the work, Analysis of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2024 Kyle Mahoney et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.



